
Nephrology
PO-145
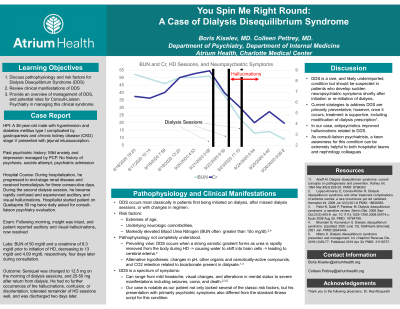

Boris Kiselev, MD
– Consult Liaison Psychiatrist and Psycho-Oncologist, Atrium Health, Charlotte, NC, United States
Colleen Pettrey, MD
– Consult Liaison Psychiatrist and Internist, Atrium Health, Charlotte, NC, United States