
Women's Mental Health
PO-144
1. Background/Significance
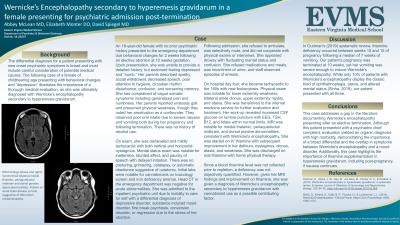
The following case of an adolescent presenting with behavioral changes and “depression” illustrates the importance of a thorough medical evaluation, as she was ultimately diagnosed with Wernicke’s encephalopathy secondary to hyperemesis gravidarum.
2. Case
An 18 year old female presented to the emergency department due to behavioral changes for two weeks following an elective abortion at ten weeks gestation. She endorsed feeling depressed, and her parents described apathy, social withdrawal, and confusion. They observed poor oral intake due to severe nausea and vomiting both during her pregnancy and following termination. Mental status examination was notable for inattention, paucity of speech, and blunted affect.
Following admission to the inpatient psychiatric unit, she was minimally cooperative, emotionally labile, and exhibited bizarre behaviors. Medically, she intermittently vomited and was incontinent of urine. Physical exam was notable for both vertical and horizontal nystagmus. She was transferred to the internal medicine service, and MRI was notable for “symmetric bilateral medial thalamic, periaqueductal midbrain and dorsal pontine signal abnormality,” consistent with Wernicke's encephalopathy. She was started on intravenous thiamine with subsequent improvement in her mental status, confusion, nystagmus, clonus, ataxia, and motor weakness.
Since a thiamine blood level was not collected prior to repletion, the cause of her symptoms cannot be definitively proven. However, given her MRI findings and her improvement following thiamine administration, Wernicke’s encephalopathy secondary to hyperemesis gravidarum was assessed to be the most likely diagnosis.
3. Discussion
In Oudman’s (2019) systematic review, thiamine deficiency occurred between weeks 10 and 15 of pregnancy following a median of 7 weeks of vomiting. Our patient’s pregnancy was terminated at 10 weeks, yet her vomiting was severe enough to induce Wernicke’s encephalopathy (WE). While only 10% of patients with WE display the classic triad of opthalmoplegia, ataxia, and altered mental status (Sinha, 2019), our patient presented with all three.
4. Conclusion/Implications
This case addresses a gap in the literature documenting WE presenting after an elective termination. Although this patient presented with a psychiatric chief complaint, evaluation yielded an organic diagnosis with high morbidity, demonstrating both the importance of a broad differential and the overlap in symptoms between Wernicke’s encephalopathy and a mood disorder. Additionally, this case underscores the importance of thiamine supplementation in hyperemesis gravidarum, including post-pregnancy if nausea persists.
5. References
Oudman, E., Wijnia, J. W., Oey, M., van Dam, M., Painter, R. C., & Postma, A. (2019). Wernicke’s encephalopathy in hyperemesis gravidarum: A systematic review. European Journal of Obstetrics & Gynecology and Reproductive Biology, 236, 84–93. https://doi.org/10.1016/j.ejogrb.2019.03.00
Sinha, S., Kataria, A., Kolla, B. P., Thusius, N., & Loukianova, L. L. (2019). Wernicke Encephalopathy—Clinical Pearls. Mayo Clinic Proceedings, 94(6), 1065–1072. https://doi.org/10.1016/j.mayocp.2019.02.018

Abbey McLean, MD
– Psychiatry Resident, Eastern Virginia Medical School, Chesapeake, VA, United StatesElizabeth Monter, DO
– Psychiatry Resident, EVMS, Norfolk, VA, United StatesDavid Spiegel, MD, FAPA
– Vice-Chairman and Professor of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, VA, United States